TLDR;
This video provides a step-by-step guide on performing a total leukocyte count (TLC) experiment, also known as white blood cell count. It covers the necessary apparatus, the procedure for collecting and diluting the blood sample, charging the Neubauer chamber, counting cells under a microscope, and performing the calculations to determine the final WBC count. Additionally, the video addresses common questions related to WBC diluting fluid composition, definitions of leukocytosis, leukopenia, and leukemia, causes of physiological leukocytosis, and potential sources of error in the experiment.
- Explains the step-by-step procedure for performing a total leukocyte count experiment.
- Covers the apparatus, sample preparation, Neubauer chamber charging, and cell counting.
- Discusses calculations, definitions of related conditions, and potential sources of error.
Introduction and Apparatus [0:00]
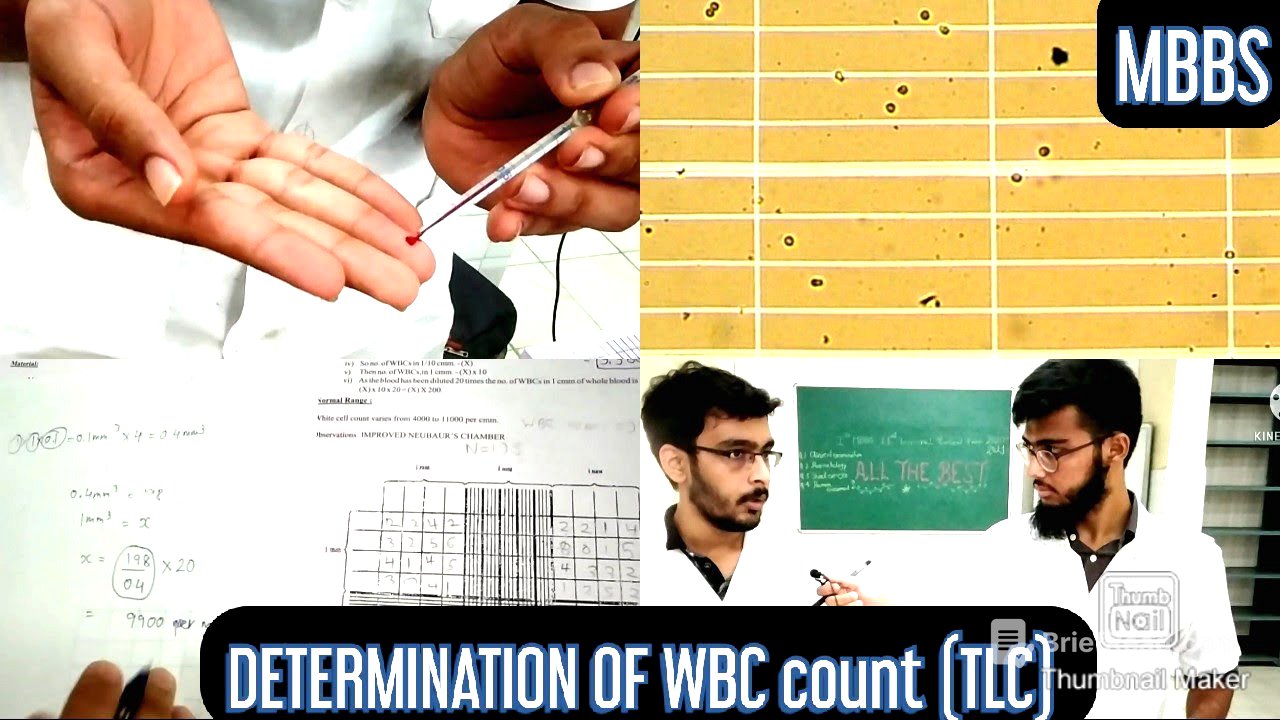
The video begins with an introduction by a first-year MBBS student who will demonstrate the total leukocyte count experiment. The required apparatus includes spirit, cotton, a lancet, Turk's fluid (WBC diluting fluid), a Neubauer chamber, and a white blood cell pipette. The Neubauer chamber being used is the improved type.
Procedure: Sterilization and Blood Collection [0:40]
The first step is to sterilize the ring finger to prevent infection. The ring finger is preferred because it is not directly connected to the bursa. A lancet is used to prick the finger, and the blood is collected using the WBC pipette up to the 0.5 mark. If excess blood enters the pipette, it can be removed by tapping the pipette against the palm. The hand and pipette tip are then cleaned with cotton.
Procedure: Dilution and Mixing [2:05]
Turk's fluid is added to the pipette up to the 11 mark to dilute the blood sample. The pipette is then held horizontally, and the fluid is mixed thoroughly by moving the arms to ensure proper dilution. A drop of the mixture is discarded to remove excess diluting fluid before charging the Neubauer chamber.
Charging the Neubauer Chamber and Settling [3:07]
A drop of the diluted blood is placed on the Neubauer chamber, allowing it to spread across the chamber via capillary action. The slide is then left to settle for one to two minutes to allow the cells to distribute evenly.
Microscopic Examination and Counting [3:38]
The Neubauer chamber is placed on the microscope, and a 10x lens is used to count the white blood cells. The WBCs are counted in the four corner squares of the chamber. The dimensions of each square are 1 mm in length and breadth, and 0.1 mm in height, resulting in a volume of 0.1 mm³. The video shows a diagram of a completed Neubauer chamber with the counted WBCs in each square.
Dilution Factor Explanation [4:35]
The video explains how a dilution factor of 20 is achieved. Starting with 0.5 ml of blood and adding diluting fluid up to the 11 ml mark results in a 1:20 dilution. This means that 1 ml of blood is diluted into 20 ml of fluid.
Calculation of WBC Count [5:01]
The volume of each Neubauer chamber square is 1 mm x 1 mm x 0.1 mm = 0.1 mm³. For the four squares counted, the total volume is 0.4 mm³. If the total number of WBCs counted in these four squares is 198, then the number of WBCs per mm³ is calculated. The calculation involves dividing the number of WBCs (198) by the volume (0.4 mm³) and then multiplying by the dilution factor (20). The final WBC count is approximately 9900 per mm³.
Composition and Function of WBC Diluting Fluid [6:16]
The WBC diluting fluid, also known as Turk's fluid, contains glacial acetic acid, methyl violet, and distilled water. Glacial acetic acid destroys the membranes of RBCs, WBCs, and platelets. Methyl violet stains the nuclei of the white blood cells, and distilled water acts as a solvent.
Definitions: Leukocytosis, Leukopenia, and Leukemia [6:43]
Leukocytosis is an increase in the WBC count, leukopenia is a decrease in the WBC count, and leukemia is an excessive number of white blood cells in the peripheral blood system. The normal range of WBCs is 4,000 to 11,000. In leukocytosis, the count exceeds 11,000; in leukopenia, it falls below 4,000; and in leukemia, it is well above 50,000.
Causes of Leukocytosis and Leukopenia [7:23]
Physiological causes of leukocytosis include pregnancy, menstruation, muscular exercise, diurnal variation, and puberty. Pathological causes include acute and chronic infections, allergic reactions, and leukemia. Pyogenic bacterial infections are the most common cause of leukocytosis. Pathological causes of leukopenia include typhoid fever, sulfa drugs, and irradiation.
WBC Production and Bead Function in Pipette [8:06]
WBCs are produced in the bone marrow. The bead in the pipette aids in mixing the blood with the diluent, helps identify the pipette (white bead for WBCs), and indicates whether the pipette is dry or wet. In a dry pipette, the bead moves freely, while in a wet pipette, it sticks to the surface.
Sources of Error and Minimization [8:37]
Possible sources of error include using a wet pipette, sucking blood beyond the 0.5 mark, formation of air bubbles, and sedimentation of RBCs. To minimize errors, ensure the pipette is clean and dry, tap the pipette against the palm to adjust the blood level, handle the blood carefully to avoid air bubbles, and roll the pipette in the palms to mix the blood and fluid well. The first few drops of the mixture are discarded because they mostly contain the diluting fluid.