TLDR;
This lecture provides an overview of the functional anatomy of the lower extremity, focusing on the hip, knee, ankle, and foot joints. It highlights the importance of understanding joint structure, function, and biomechanics for optimizing performance, preventing injuries, and guiding rehabilitation. The lecture also covers the kinetic chain, injury prevention strategies, the role of footwear, and future trends in the field.
- Functional anatomy of lower extremity is crucial for weightbearing, locomotion, and athletic performance.
- Joint coordination is essential for efficiency and injury prevention.
- Strength and proprioceptive training, along with proper footwear, are key to preventing injuries.
Introduction [0:15]
The lecture introduces the functional anatomy of the lower extremity, emphasizing its role in weightbearing, locomotion, and athletic performance. It highlights the importance of understanding the anatomy of the hip, knee, ankle, and foot joints for optimizing performance, preventing injuries, and guiding rehabilitation. The lecture will focus on functional rather than structural intricacies.
Overview of Lower Extremity Joints [1:52]
The hip joint is a ball and socket joint that allows multidirectional movement. The knee joint is a hinge joint with limited rotation. The ankle joint primarily allows dorsiflexion and plantar flexion. The foot and toe joints are critical for balance, propulsion, and force absorption.
Hip Joint: Structure, Function, and Biomechanics [2:37]
The hip joint, or femoral acetabular joint, is formed by the head of the femur and the acetabulum. Key ligaments include the iliofemoral (prevents hyperextension), pubofemoral (limits excessive abduction), and ischiofemoral (reinforces the posterior hip). Movements include flexion, extension, abduction, adduction, internal and external rotation, and circumduction. Muscles involved in flexion are the iliosus, rectus femoris, and sartorius; extension involves the gluteus maximus and hamstrings (biceps femoris, semitendinosis, semimebranosus); abduction is performed by the gluteus medius and minimus, which also prevent hip drop in single leg stance; adduction is done by the adductor longus, brevis, and magnus, with assistance from the gracilis and pectineus. Load distribution varies with activity, and hip abductors stabilize the pelvis. Common injuries include labral tears, femoroacetabular impingement (FAI), hip dislocations, and trochanteric bursitis.
Knee Joint: Structure, Function, and Biomechanics [5:09]
The knee joint is a hinge joint allowing limited rotation, with articulating surfaces including the femur, tibia, and patella. Ligaments include the anterior cruciate ligament (ACL) preventing anterior tibial translation, posterior cruciate ligament (PCL) preventing posterior tibial translation, medial collateral ligament (MCL), and lateral collateral ligament (LCL) providing medial and lateral stability. The medial and lateral menisci act as shock absorbers and improve joint congruency. Movements include flexion, extension, and limited internal and external rotation. Flexors are the hamstrings (biceps femoris, semitendinosus, semimembranosus) assisted by the gastrocnemius. Extensors are the quadriceps (rectus femoris, vastus lateralis, vastus medialis, vastus intermedius). The popliteus unlocks the knee, and the sartorius causes medial rotation. The quadriceps-hamstring ratio (Q ratio) is crucial for knee stability, ideally 60:40. The patella acts as a lever to improve quadriceps efficiency. Common injuries include ACL rupture, meniscal tears, and patellar tendinopathy.
Ankle Joint: Structure, Function, and Biomechanics [7:47]
The ankle joint, or talocrural joint, is a hinge joint comprising the tibia, fibula, and talus. The medial deltoid ligament provides stability against eversion, while the lateral ATFL, CFL, and PTFL prevent excessive inversion. Movements include dorsiflexion, plantar flexion, inversion, and eversion. Dorsiflexors include the tibialis anterior, extensor hallucis longus, and extensor digitorum longus. Plantar flexors include the gastrocnemius, soleus, and tibialis posterior. Inverters are the tibialis posterior and flexor hallucis longus, while everters are the peroneus longus and peroneus brevis. The ankle joint is crucial for gait and shock absorption, with stability affected by muscle strength, proprioception, and ligament integrity. Common injuries include lateral ankle sprains, Achilles tendon ruptures, and high ankle sprains.
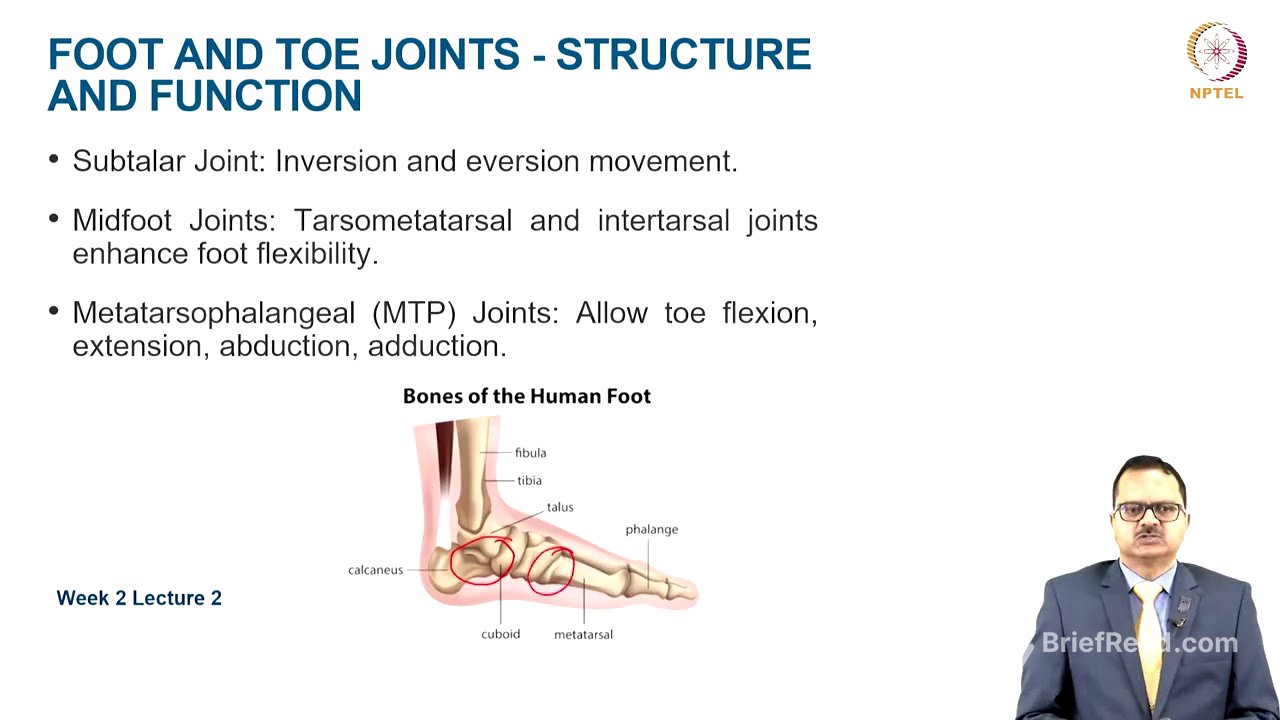
Foot and Toe Joints: Structure, Function, and Biomechanics [9:32]
The subtalar joint facilitates inversion and eversion movements. Midfoot joints like the tarsometatarsal and intertarsal joints enhance foot flexibility. Metatarsophalangeal joints allow toe flexion, extension, abduction, and adduction. Intrinsic muscles include the lumbricals and interossei, while the plantar fascia supports the foot arches. Extrinsic muscles like the tibialis posterior, peroneals, and gastrocnemius influence arch height. Arch stability is provided by the medial longitudinal, lateral longitudinal, and transverse arches, which offer stability and shock absorption. Pronation involves eversion, abduction, and dorsiflexion, while supination involves inversion, adduction, and plantar flexion. These movements help distribute ground reaction forces during walking and running. Common injuries include plantar fasciitis, stress fractures, and hallux valgus.
Kinetic Chain Relationship [12:36]
All joints, tendons, and ligaments are connected via the kinetic chain. Improper foot biomechanics can affect knee and hip function. Weak glutes contribute to knee valgus and instability. Overactive hip flexors limit hip extension and cause lower back pain. Weak gluteals may lead to excessive knee valgus and osteoarthritis.
Injury Prevention Strategies [13:21]
Strength training and proprioception exercises improve joint stability, balance, and neuromuscular control. Proper footwear selection reduces injury risk. Custom orthotics can correct biomechanical errors in the foot and ankle.
Future Trends and Targeted Prevention Program [14:03]
Wearable technology is increasingly used for biomechanics assessment, with markerless assessments becoming more common. Regenerative medicine is advancing, especially for osteoarthritis. AI-driven rehab programs allow for minute adjustments based on athlete performance. 3D-printed orthotics provide accurate anatomical support. Genetic profiling is being used for injury risk prevention. A targeted prevention program includes warm-up, stretching, strengthening exercises, balance and proprioception training, structured multimodal training, nutritional strategies (increased protein, calcium, vitamin D, B12, magnesium, zinc, and fluids), technique modification, shoe and equipment modification, and load management.
Take Home Message [16:23]
The lower extremity is essential for weightbearing, mobility, and stability. Hip flexors, extensors, abductors, and adductors are crucial. The quadriceps-hamstring ratio is vital for knee stability. Ankle and foot muscles support movement and stability through arches. Joint coordination prevents injuries like ACL tears, ankle sprains, and plantar fasciitis. Strength training, proprioceptive training, and phased rehabilitation optimize function and recovery.