TLDR;
Dr. Lewinsky's presentation focuses on raising awareness about ATTR amyloidosis, emphasizing the importance of early diagnosis and treatment to improve patient outcomes and quality of life. The discussion covers the nature of amyloid, its effects on the heart and other organs, diagnostic methods, treatment options, and patient expectations. It highlights the complexities in diagnosing ATTR amyloidosis due to its varied presentations and the need for a multidisciplinary approach.
- ATTR amyloidosis is often misdiagnosed due to its diverse symptoms and the current siloed approach in medical practice.
- Non-invasive diagnostic tools like PYP imaging have revolutionized the diagnosis of cardiac amyloidosis.
- New therapies, including stabilizers and silencers, offer hope for modifying the disease and improving patient outcomes.
Introduction [0:14]
Dr. Lewinsky expresses his pleasure in working with the amyloid support group and emphasizes the unique and close relationships that amyloidologists develop with their patients and families. He highlights the importance of communication and information sharing in managing amyloidosis effectively. As the head of nuclear cardiology and the amyloid clinic, he is actively involved in both the diagnosis and management of patients with amyloidosis. The goal of the presentation is to increase awareness of ATTR amyloidosis, promote appropriate testing, and ultimately lead to earlier diagnosis, treatment, and improved quality of life for patients.
Vignette: A Missed Diagnosis [1:24]
Dr. Lewinsky shares a case of a 76-year-old afro-caribbean male who was initially misdiagnosed despite showing several red flags indicative of cardiac amyloidosis. The patient presented with symptoms such as abdominal pain, weight loss, shortness of breath, and neuropathy, but was discharged without proper testing or a clear diagnosis. Despite referrals to multiple specialists, the underlying cause of his heart disease was not identified, leading to a delayed diagnosis of amyloidosis. By the time Dr. Lewinsky saw him, the disease had progressed too far, and the patient died within three months, highlighting the critical need for early detection and intervention.
What is Amyloid? [4:22]
The presentation addresses the fundamental questions about amyloidosis, including its nature, effects on the heart, involvement of other organs, diagnostic methods, treatment options, and patient expectations. Amyloidosis is characterized by the misfolding and aggregation of proteins into fibrils that deposit in various tissues and organs, disrupting their normal function. Understanding these aspects is crucial for patients and their families to effectively interact with clinicians and manage the disease.
Types of Amyloidosis: AL vs. ATTR [5:10]
The discussion focuses on the two major types of amyloidosis: AL (light chain) amyloidosis and ATTR (transthyretin) amyloidosis, with a primary focus on ATTR amyloidosis. ATTR amyloidosis involves the transthyretin protein, normally produced in the liver to transport thyroxine and retinol. This protein undergoes a transformation, forming fibrils that infiltrate tissues, particularly the heart, leading to various diseases. The process involves the breakdown of the transthyretin tetramer into monomers, which then clump together to form amyloid deposits.
ATTR Amyloidosis in America [6:51]
In America, ATTR amyloidosis is the most common form, particularly the wild-type, affecting mostly males in the Medicare age population, around 76 years old. These individuals typically have a thickened heart and a septum that is more than one and a half times the normal size. Hereditary amyloid is less common but seen in specific populations, such as African Americans, who may carry the gene for the V122I mutation. The presentation of hereditary ATTR can vary, with some forms predominantly affecting the nervous system and others the heart, though most patients experience a mix of both cardiac and neurologic involvement.
Challenges in Diagnosing Amyloidosis [8:50]
One of the main reasons for the difficulty in diagnosing amyloidosis is the siloed approach in modern medical practice, where specialists focus on their specific areas without considering the systemic nature of the disease. This lack of a comprehensive view can lead to missed red flags and delayed diagnoses. It is crucial to recognize that amyloidosis is a multi-organ disease, and healthcare providers need to look beyond their individual scope of expertise to identify potential cases early on.
Is Amyloidosis a Rare Disease? [9:37]
While amyloidosis is often considered a rare disease, data suggests that ATTR amyloidosis is more prevalent than previously thought, especially in the elderly. It is found in a significant percentage of patients over 85 who undergo autopsies and in a notable proportion of individuals with heart failure with preserved ejection fraction. Studies using PYP imaging have also revealed that a considerable number of patients hospitalized with heart failure or undergoing TAVR procedures test positive for ATTR amyloidosis, indicating that it may not be as rare as commonly believed. As age increases, the likelihood of finding amyloid also increases, with up to 40% of patients over 80 being diagnosed with the condition.
Cardiac Manifestations of Amyloidosis [11:32]
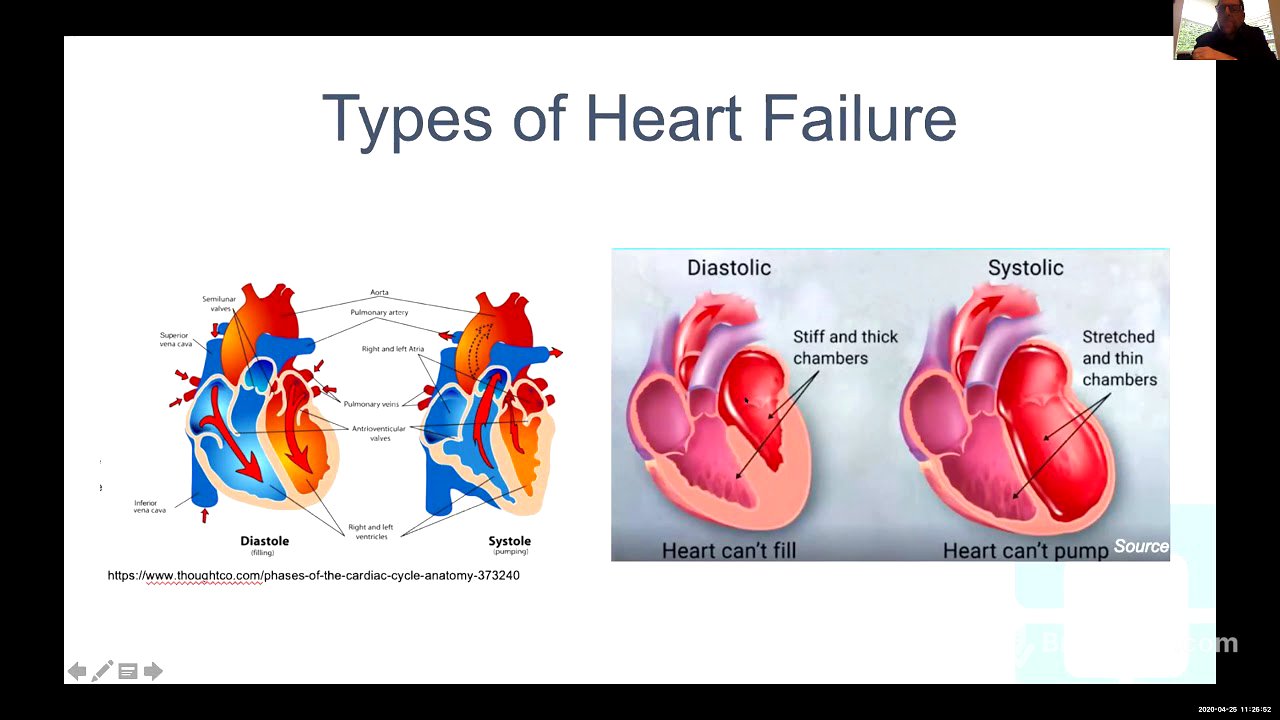
Cardiac manifestations of amyloidosis include congestive heart failure, atrial fibrillation, slow heart rate or conduction diseases requiring a pacemaker, and an increased risk of sudden death. As the disease progresses, it can lead to cardiorenal syndrome, where the heart and kidneys negatively affect each other, resulting in a decline in both cardiac and renal function. The heart's primary function is to pump blood to the organs, and heart failure occurs when it cannot pump an adequate amount of blood or requires too much pressure to do so, leading to symptoms like shortness of breath.
Microscopic View of Amyloid [13:19]
Microscopically, amyloid deposits appear as fibrils interspersed between the heart muscle cells (myocytes). These fibrils can be identified using Congo red staining, which highlights them as large fibers infiltrating the tissue. When viewed under a polarized microscope, these deposits exhibit a characteristic apple-green birefringence, a typical and diagnostic finding for amyloidosis. While a biopsy can be a reliable method for diagnosis, the goal is to achieve a diagnosis without resorting to a myocardial biopsy.
Cardiac Abnormalities [14:00]
An amyloid heart typically exhibits thickening of both the left and right ventricles, enlargement of the left and right atria, and thickening of the intra-atrial septum. The leaflets of the mitral valve also become thickened. These abnormalities can be observed on echocardiography or cardiac MRI, which are suggestive but not definitive for diagnosis. In addition to heart failure, amyloidosis can cause various electrical abnormalities, such as right or left bundle branch blocks, impaired conduction leading to a very slow heart rate, and atrial fibrillation.
Non-Cardiac Symptoms of Amyloidosis [15:21]
Amyloidosis is a multi-organ disease with a wide range of non-cardiac symptoms, making it a "great masquerader." Carpal tunnel syndrome is a common finding, with 50% of patients with ATTR amyloidosis having a history of bilateral carpal tunnel syndrome, often occurring years before cardiac symptoms. Other symptoms include lumbar spinal stenosis, neuropathy with numbness and tingling in the legs, floaters, and gastrointestinal issues such as poor appetite, constipation, and diarrhea. Autonomic dysfunction, leading to blood pressure drops and dizziness upon standing, urinary retention, and sexual dysfunction are also common. The rapid progression of these symptoms, often more pronounced than in typical heart failure or neuropathy, should raise suspicion for amyloidosis.
Diagnostic Challenges and Red Flags [18:42]
Diagnosing amyloidosis has been challenging due to the lack of organized diagnostic approaches and effective treatments. Patients often see multiple doctors and cardiologists before receiving a correct diagnosis. Red flags such as carpal tunnel syndrome and lumbar stenosis should prompt further investigation. If a patient undergoes surgery for lumbar stenosis, the pathology lab should be asked to stain the tissue for amyloid.
Cardiac Testing: ECG and Echocardiogram [20:08]
Traditional cardiac testing includes electrocardiograms (ECG) and echocardiograms. An ECG may show low voltage, while an echocardiogram reveals a thickened heart. The combination of low voltage on the ECG and a thickened heart on the echocardiogram is suggestive, but not diagnostic, of amyloidosis. Strain imaging, a newer tool used with echocardiography, can show a characteristic "cherry on top" pattern, where the strain is preserved at the apex of the heart while reduced in other areas, further indicating amyloidosis.
PYP Imaging for Cardiac Amyloidosis [22:07]
PYP (pyrophosphate) imaging has revolutionized the diagnosis of cardiac amyloidosis. This non-invasive test involves injecting a safe tracer that binds to amyloid deposits in the heart. The uptake of the tracer is measured using a semi-quantitative scale, with grades of 2 or 3 being diagnostic of amyloidosis. Quantitative measurements can also be made by comparing the tracer uptake in the heart to the uptake in the chest. While high levels of uptake are typically consistent with wild-type ATTR amyloid, it is essential to rule out AL amyloidosis.
Diagnostic Process for ATTR Amyloidosis [25:25]
The diagnostic process for ATTR amyloidosis begins with an ECG and echocardiogram, followed by ruling out AL amyloidosis. If the pyrophosphate scan is positive, the diagnosis of ATTR amyloidosis is made. Genetic testing is then performed to determine whether it is the wild-type or hereditary form.
Medical Therapy for Amyloidosis [26:06]
Effective medical therapy for amyloidosis requires careful management, often best achieved at a cardiac amyloid center. Diuretics like torsamide or bumetadine are preferred over furosemide due to better absorption. Patients are taught to adjust their diuretic dosage to manage fluid retention. Aldactone is used to prevent atrial fibrillation and remodeling. Traditional heart failure medications like ACE inhibitors, angiotensin receptor blockers, and beta-blockers are generally avoided or used cautiously, as they may not be well-tolerated in patients with amyloidosis. Patients with amyloidosis are highly sensitive to volume changes, requiring careful monitoring to avoid dehydration.
Atrial Fibrillation and Advanced Therapies [30:17]
Atrial fibrillation is a common presentation of ATTR amyloidosis, often difficult to control with standard treatments. Patients with atrial fibrillation require anticoagulants to reduce the risk of stroke. Liver transplants or combined liver-heart transplants are being used in advanced cases, particularly those with the V30 mutation.
Disease-Modifying Therapies [31:37]
The era of therapeutic nihilism is over, with new disease-modifying therapies available for ATTR amyloidosis. These therapies include silencers that block protein development, stabilizers that prevent the tetramer from breaking down, and potential future treatments that eliminate amyloid fibers. Patisiran and inotersen are silencers approved for hereditary polyneuropathy, while tafamidis is a stabilizer approved for both wild-type and hereditary cardiomyopathy.
Available Drugs [32:05]
Patisiran, an RNA interfering agent, and inotersen, an antisense oligonucleotide, prevent the formation of abnormal transthyretin. Patisiran is given every three weeks via infusion, while inotersen is given at home via subcutaneous injections. Tafamidis stabilizes the transthyretin tetramer, preventing it from breaking down and forming fibrils. Clinical trials have shown that tafamidis improves survival and quality of life in patients with ATTR amyloidosis.
Additional Therapies and Ongoing Research [36:39]
Other potential therapies include diflunisal, a non-steroidal anti-inflammatory drug, green tea extracts, and doxycycline combined with tudca. Ongoing research includes studies on patisiran, vutrisiran, and a subcutaneous injection similar to inotersen. AG-10, another stabilizer, and PRX, an antibody, are also being investigated. An international registry has been started to study the relationship between amyloid and coronavirus.
Amyloid Center and Facebook Site [39:21]
The Cleveland Clinic jointly runs an amyloid center in Florida and Cleveland. A Cleveland Clinic Facebook site provides supplementary information and a way to communicate with others. The center works with the Amyloid Support Group to provide additional resources and support.