TLDR;
This video provides a detailed explanation of upper motor neuron (UMN) versus lower motor neuron (LMN) lesions, central versus peripheral facial palsy, and the unique innervation patterns of the 11th and 12th cranial nerves. It covers the anatomy and function of the corticospinal and corticobulbar tracts, differences between UMN and LMN lesions in terms of muscle bulk, tone, reflexes, and fasciculations. Additionally, it explains the concept of bilateral innervation of cranial nerves, the exception of the 7th cranial nerve in UMN lesions, and the peculiarities of the 11th and 12th cranial nerves.
- UMN lesions typically present with spasticity, brisk reflexes, and extensor plantar response, while LMN lesions show flaccidity, absent reflexes, and fasciculations.
- Central facial palsy affects the lower part of the face contralaterally due to unilateral innervation of the lower facial nucleus, whereas peripheral facial palsy affects the entire ipsilateral face.
- The 11th and 12th cranial nerves have unique innervation patterns, with the sternocleidomastoid muscle having ipsilateral cortical control and the genioglossus muscle having contralateral control.
Introduction to Upper and Lower Motor Neuron Lesions [0:52]
The video introduces the fundamental concepts of upper motor neuron (UMN) and lower motor neuron (LMN) lesions, which are essential for understanding central versus peripheral facial palsy. The corticospinal and corticobulbar tracts, collectively known as the pyramidal tract, are responsible for voluntary movements. The UMN consists of cortical bulbar fibers that extend from the cortex to the motor part of the cranial nerve nuclei, and corticospinal fibers that extend from the cortex to the anterior horn cells of the spinal cord. The LMN includes cranial nerves emerging from the cranial nerve nuclei and peripheral nerves originating from the anterior horn cells.
Pyramidal Tract and Cranial Nerve Innervation [3:12]
The pyramidal tract is purely a motor pathway, innervating the motor components of cranial nerve nuclei, specifically the 3rd, 4th, motor part of the 5th, 6th, 7th, 10th, 11th, and 12th cranial nerves. It does not innervate sensory nerves like the 8th cranial nerve. A key concept is that most cranial nerve nuclei receive bilateral innervation from both sides of the cortex. This bilateral innervation explains why lesions above the brainstem typically result in contralateral hemiplegia without affecting cranial nerve function, except for the 7th cranial nerve.
Upper Motor Neuron vs. Lower Motor Neuron Lesions: Key Differences [5:52]
The video outlines the key differences between UMN and LMN lesions. In UMN lesions, muscle bulk is generally normal with possible disuse atrophy, while LMN lesions exhibit significant muscle wasting. Muscle tone is increased (hypertonia, either spasticity or rigidity) in UMN lesions and decreased (hypotonia) in LMN lesions. Superficial reflexes are absent in both UMN and LMN lesions. Deep tendon reflexes are brisk in UMN lesions due to disinhibition and absent in LMN lesions. The Babinski sign (extensor plantar response) is present in UMN lesions and absent or flexor in LMN lesions.
Muscle Weakness and Fasciculations [8:45]
In UMN lesions, groups of muscles are affected, leading to characteristic patterns like flexion of the upper limb and extension of the lower limb, resulting in a circumduction gait. In LMN lesions, individual muscles are affected based on specific nerve root involvement. Fasciculations, involuntary muscle twitchings, are present in LMN lesions due to denervation supersensitivity, where the anterior horn cells become hypersensitive to acetylcholine.
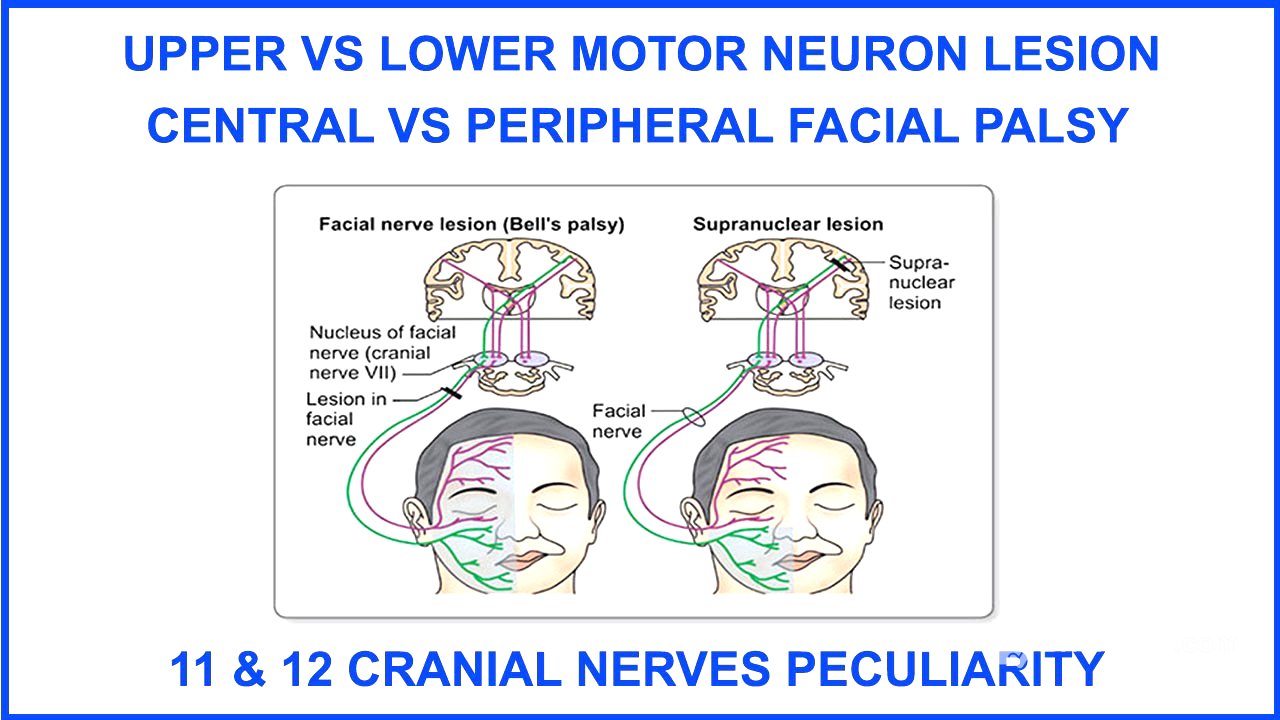
Central vs. Peripheral Facial Palsy: The 7th Cranial Nerve [10:33]
The video explains why the 7th cranial nerve is uniquely affected in lesions above the brainstem. The facial nerve nucleus in the pons has an upper and lower part. The upper part of the facial nucleus, which supplies the upper face, receives bilateral innervation, while the lower part, which supplies the lower face, receives only contralateral innervation. Therefore, in a UMN lesion, only the lower part of the contralateral face is affected because the upper part is compensated by bilateral innervation. In contrast, LMN lesions affect the entire ipsilateral face because the lesion is at or below the facial nerve nucleus, disrupting both upper and lower facial muscles.
Bell's Phenomenon and Corneal Reflex [13:38]
Bell's phenomenon, the upward gaze of the eyeball with forceful eyelid closure, is a normal reflex. In peripheral facial palsy (LMN lesion), Bell's phenomenon is more apparent because the patient cannot close their eyelid due to orbicularis oculi weakness, revealing the upward movement of the eyeball when they attempt to close their eye. The corneal reflex, involving the ophthalmic division of the trigeminal nerve (afferent) and the facial nerve (efferent), is present in UMN lesions but absent in LMN lesions due to facial nerve involvement affecting the orbicularis oculi muscle.
Facial Reflexes and Emotional Dissociation [17:31]
Facial reflexes, such as the orbicularis oculi reflex, are brisk in UMN lesions and diminished or absent in LMN lesions. The supranuclear pathway for facial movement includes both voluntary and emotional components. In UMN lesions, there can be voluntary-emotional dissociation, where a person may have difficulty showing their teeth on command (voluntary) but can smile normally in response to an emotional stimulus, or vice versa. This dissociation does not occur in LMN lesions, where both voluntary and emotional facial movements are affected.
Peculiarities of the 11th and 12th Cranial Nerves [19:41]
The video highlights exceptions to the general rule of bilateral innervation of cranial nerves, focusing on the 11th and 12th cranial nerves. The 11th cranial nerve, which innervates the sternocleidomastoid muscle, has predominantly ipsilateral innervation. A right cortical lesion affects the ipsilateral (right) sternocleidomastoid, impairing the ability to turn the head to the opposite (left) side. The 12th cranial nerve, specifically the genioglossus muscle, has predominantly contralateral innervation. A right cortical lesion affects the contralateral (left) genioglossus, causing the tongue to deviate towards the same side as the lesion (right) upon protrusion.

![불손한 부하직원 다루는 법 [유세미의 직장수업 TV]](https://wm-img.halpindev.com/p-briefread_c-10_b-10/urlb/aHR0cDovL2ltZy55b3V0dWJlLmNvbS92aS9ILTJ2SDBLcS1udy9ocWRlZmF1bHQuanBn.jpg)