TLDR;
This video provides an overview of the pharmacology of drugs used to treat pituitary and thyroid disorders. It covers the roles of the hypothalamus and pituitary gland in the endocrine system, detailing how hormones regulate various bodily functions. The lecture explains the mechanisms of action for drugs targeting thyroid hormones, gonadotropins, adrenal hormones, growth hormones, prolactin, vasopressin, and oxytocin.
- Hypothalamus and pituitary gland are key players in the endocrine system.
- Hormones regulate metabolism, growth, and reproduction.
- Drugs mimic or block hormone effects to treat endocrine disorders.
Hypothalamus & Pituitary [0:02]
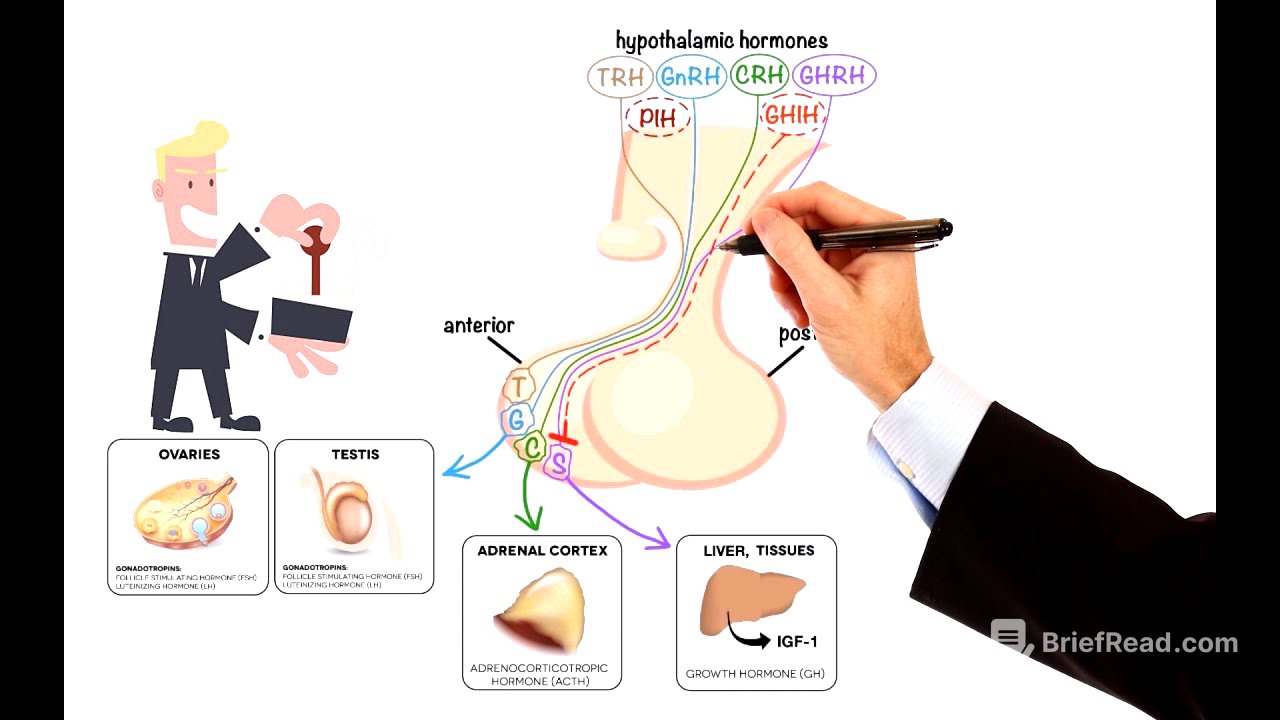
The hypothalamus and pituitary gland are central to the endocrine system. The pituitary, controlled by the hypothalamus, regulates hormone secretion. Hormones act as chemical messengers, influencing bodily functions. Imbalances can lead to medical issues. The pituitary has two lobes: the anterior lobe, which produces hormones in response to hypothalamic hormones, and the posterior lobe, which directly secretes hormones produced in the hypothalamus. Hypothalamic hormones include those that stimulate the anterior pituitary, such as thyrotropin-releasing hormone (TRH), gonadotropin-releasing hormone (GnRH), corticotropin-releasing hormone (CRH), and growth hormone-releasing hormone (GHRH), as well as inhibiting hormones like growth hormone-inhibiting hormone (GHIH) and prolactin-inhibiting hormone (PIH).
Anterior pituitary [1:02]
Hypothalamic hormones act on the anterior pituitary gland. Thyrotropin-releasing hormone (TRH) stimulates thyrotrophs to release thyroid-stimulating hormone (TSH), which then stimulates the thyroid gland to produce thyroid hormones. Gonadotropin-releasing hormone (GnRH) stimulates gonadotrophs to release follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which affect the ovaries and testes. Corticotropin-releasing hormone (CRH) stimulates corticotrophs to release adrenocorticotropic hormone (ACTH), which stimulates the adrenal cortex. Growth hormone-releasing hormone (GHRH) stimulates somatotrophs to release growth hormone (GH), which stimulates the liver to produce insulin-like growth factors. Growth hormone-inhibiting hormone (GHIH) inhibits growth hormone release, and prolactin-inhibiting hormone (PIH), or dopamine, inhibits prolactin secretion.
Posterior pituitary [2:38]
The posterior pituitary releases hormones synthesized in the hypothalamus. These hormones include anti-diuretic hormone (ADH), which regulates water balance in the kidneys, and oxytocin, which regulates uterine contractions and milk ejection. These hormones play a crucial role in regulating metabolism, growth, and reproduction. Drugs have been developed to mimic or block their effects to treat various endocrine disorders.
Thyroid hormones [3:24]
Thyroid hormones are synthesized in the thyroid follicle, which contains colloid and follicular cells. Thyroglobulin, a glycoprotein, and iodide are essential ingredients. Iodide is actively transported into the cell and then into the colloid. Thyroid peroxidase oxidizes iodide to iodine, which is added to tyrosyl residues on thyroglobulin in a process called iodination. Adjacent tyrosyl residues are paired together, and the complex re-enters the follicular cell. Proteolytic enzymes digest thyroglobulin, releasing thyroxine (T4) and triiodothyronine (T3) into the circulation. T4 and T3 bind to carrier proteins for transport to target cells. Inside the target cell, T4 is converted to T3 by deiodinase enzymes D1 and D2, increasing the levels of the active hormone. Deiodinase 3 (D3) inactivates T4 by converting it to reverse T3 (rT3). T3 binds to thyroid hormone receptors (TR) in the nucleus, forming heterodimers with the retinoid X receptor (RXR) to induce transcription of target genes.
Drugs for thyroid disorders include those for hypothyroidism and hyperthyroidism. Hypothyroidism is treated with Levothyroxine (synthetic T4), Liothyronine (synthetic T3), Liotrix (synthetic T4 and T3 combination), and desiccated natural thyroid (natural T4 and T3 mix). Hyperthyroidism is treated with Propylthiouracil and Methimazole, which inhibit thyroid peroxidase and coupling of iodotyrosines. Propylthiouracil also inhibits deiodinase 1 (D1), preventing T4 to T3 conversion.
Gonadotropins [7:27]
Gonadotropin-releasing hormone (GnRH) is released in a pulsatile manner and binds to receptors on pituitary gonadotrophs. The frequency of GnRH pulses regulates the secretion of LH and FSH. GnRH analogs modulate GnRH effects. GnRH agonists like Goserelin, Histrelin, Leuprolide, and Nafarelin initially stimulate LH and FSH secretion, followed by downregulation of the pituitary-gonadal axis. GnRH antagonists like Degarelix, Elagolix, Ganirelix, and Cetrorelix suppress pituitary gonadotropins by blocking GnRH receptors, avoiding the initial stimulatory phase. This leads to inhibition of estrogen and androgen synthesis, effective in treating hormone-sensitive cancers and gynecological disorders. Pharmaceutical preparations of LH and FSH, including Menotropins (LH and FSH mixture), Urofollitropin (purified FSH), Follitropin (recombinant FSH), Lutropin (recombinant LH), and Choriogonadotropin alfa (recombinant hCG), stimulate spermatogenesis in men and induce follicle development and ovulation in women.
Adrenal hormones [10:09]
Adrenocorticotropic hormone (ACTH) stimulates the synthesis and release of adrenocortical and androgen hormones. ACTH activates cholesterol side-chain cleavage enzyme, converting cholesterol to pregnenolone, the precursor of mineralocorticoids, glucocorticoids, androgens, and estrogens. Adrenal gland disorders include hormone deficiency and excess. Addison’s disease, an adrenocortical insufficiency, is treated by replacing missing aldosterone with Fludrocortisone and missing cortisol with Hydrocortisone or Prednisone. Cushing’s syndrome, characterized by excessive cortisol production, is treated by stopping causative corticosteroid medications or, in the case of adrenal tumors, using Ketoconazole, Mitotane, and Metyrapone to inhibit cortisol synthesis enzymes.
Growth hormones [11:46]
Growth hormone (somatotropin) stimulates the liver and other tissues to secrete insulin-like growth factor-1 (IGF-1), which promotes cartilage and bone growth, as well as protein formation in skeletal muscle. Growth hormone also directly binds to target cells, breaking down triglycerides and suppressing lipid accumulation in fat cells. Growth hormone deficiency can lead to growth retardation or dwarfism, treated with synthetic somatotropin. Pediatric patients unresponsive to somatotropin can be treated with Mecasermin, a recombinant human IGF-1 product. Somatostatin, or growth hormone-inhibiting hormone, inhibits the pituitary gland's secretion of growth hormone. Excessive growth hormone secretion, leading to gigantism in children and acromegaly in adults, can be managed with synthetic somatostatin forms like Octreotide and Lanreotide, which inhibit growth hormone secretion by binding to somatostatin receptors.
Prolactin [14:05]
Prolactin secretion is regulated by dopamine, which inhibits prolactin secretion by acting on lactotrophs through D2-receptors. Prolactin disorders include insufficient levels, leading to failure to lactate, and excessive levels, leading to galactorrhea and infertility. Dopamine receptor antagonists like Metoclopramide increase prolactin secretion by blocking D2 receptors. Dopamine receptor agonists like Bromocriptine and Cabergoline inhibit prolactin secretion by stimulating D2 receptors.
Vasopressin [15:05]
Vasopressin, or anti-diuretic hormone (ADH), is released in response to changes in plasma osmolality, volume, or blood redistribution. It binds to V2 receptors (V2R) in the kidneys, stimulating the insertion of aquaporins into the luminal membrane, allowing water reabsorption. Vasopressin also binds to V1 receptors (V1R) on vascular smooth muscle, causing vasoconstriction. Therapeutic options include natural vasopressin and Desmopressin (DDAVP), a selective V2 receptor agonist, used to treat diabetes insipidus, bleeding disorders, and nocturnal enuresis. Vasopressin receptor antagonists like Conivaptan and Tolvaptan block V2 receptors, correcting hyponatremia due to the syndrome of inappropriate secretion of antidiuretic hormone.
Oxytocin [16:51]
Oxytocin plays roles in female reproduction. Stretching of the uterus and cervix stimulates oxytocin secretion, causing uterine contractions during labor. After birth, suckling stimulates oxytocin release, causing milk ejection. Exogenous oxytocin can be administered to induce labor and inhibit postpartum bleeding.