TLDR;
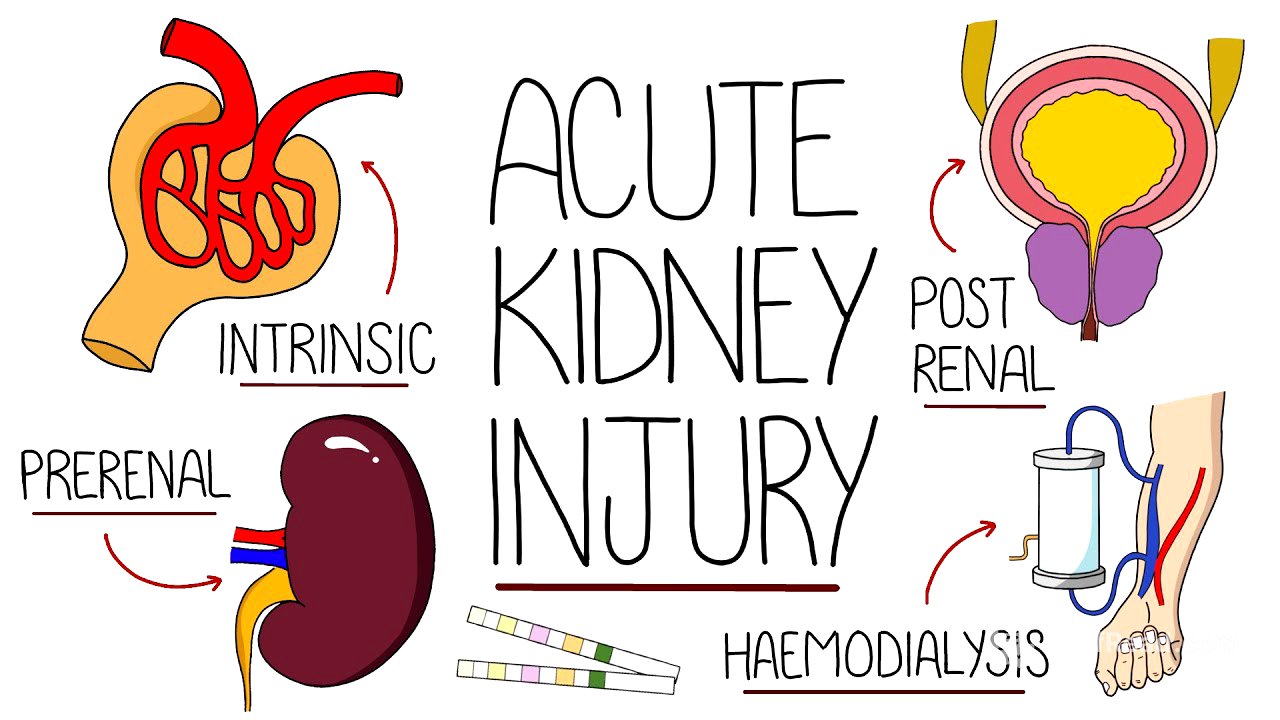
Okay, so this video gives a breakdown of acute kidney injury (AKI), also known as acute renal failure. It covers what AKI is, how it's diagnosed using GFR, the different causes (pre-renal, intrinsic, and post-renal), symptoms, diagnosis methods, and finally, the treatment approaches. Key takeaways include understanding the importance of GFR, recognizing the various causes of AKI, and knowing the treatment options available.
- AKI is a sudden decline in kidney function, measured by GFR.
- Causes are categorized into pre-renal (reduced blood flow), intrinsic (direct kidney damage), and post-renal (obstruction).
- Diagnosis involves blood tests (creatinine, electrolytes), urine studies, and imaging.
- Treatment focuses on addressing the underlying cause, fluid management, and correcting electrolyte imbalances; renal replacement therapy may be needed.
What is an Acute Kidney Injury? [0:00]
The video starts off by explaining that acute kidney injury (AKI), sometimes called acute renal failure, is basically when your kidneys suddenly stop working as well as they should. To figure out how well the kidneys are working, doctors use something called the glomerular filtration rate, or GFR. This measures how well your kidneys are filtering your blood. The nephron, which has the glomerulus, filters waste into the Bowman's capsule. GFR measures the volume filtered through the glomerulus into the Bowman's capsule in a given time.
Glomerular Filtration Rate (GFR) Explained [0:20]
The GFR is a measure of how well the kidneys filter blood. The functional unit doing the filtering is the nephron, which includes the glomerulus. The filtrate passes through different parts of the nephron (proximal convoluted tubule, Loop of Henle, distal convoluted tubule, and distal collecting duct) where secretion and reabsorption happen, eventually forming urine. Since directly measuring GFR is tough, creatinine clearance is used to estimate it. Creatinine, a breakdown product from muscle tissue, is filtered by the glomerulus but also secreted, which can slightly overestimate GFR. Formulas like the Cockcroft-Gault formula and the modification of diet in renal disease (MDRD) study group formula are used to estimate GFR, considering factors like age, mass, gender, and serum creatinine.
Acute Kidney Injury Causes – Prerenal [2:12]
The video then breaks down the causes of AKI into three main categories: pre-renal, intrinsic, and post-renal. Pre-renal causes are all about reduced blood flow to the kidneys. This can happen due to things like hypovolemia (from vomiting, diarrhea, hemorrhages, or burns), hypotension (caused by hypovolemia, cardiogenic issues, distributive problems like sepsis or anaphylaxis, or obstructive issues like a pulmonary embolism), renal artery stenosis, or aortic dissection. Basically, anything that messes with the blood supply to the kidneys falls into this category.
Acute Kidney Injury Causes – Intrinsic [2:59]
Intrinsic causes of AKI involve direct damage to the nephron. This includes things like non-steroidal anti-inflammatory drugs (NSAIDs) causing afferent arterial vasoconstriction, ACE inhibitors or angiotensin receptor blockers (ARBs) causing efferent vasodilation, both reducing GFR. Acute tubular necrosis (ATN) happens when the epithelial cells of the tubular system die, which can be caused by pre-renal injury, rhabdomyolysis, hemolysis, antibiotics like aminoglycosides and vancomycin, and contrast from radiological studies. Acute interstitial nephritis (AIN) is inflammation of the kidney's interstitium, caused by medications like antibiotics (penicillins), proton pump inhibitors (PPIs), NSAIDs, and immune diseases like lupus. Glomerular diseases like anti-glomerular basement membrane disease (Goodpasture's disease) or post-infection glomerulonephritis, and vascular conditions like thrombosis or embolic events can also cause intrinsic AKI.
Acute Kidney Injury Causes – Postrenal [4:46]
Post-renal causes are due to obstruction of urine flow after the kidneys. This can be from things outside the urinary system, like benign prostatic hypertrophy (BPH) or tumors pressing on the ureters. It can also be from things inside the urinary system, like strictures, intrinsic tumors, or renal stones. However, kidney stones usually only affect one kidney, so they're a less common cause of AKI.
Acute Kidney Injury Symptoms [5:18]
There aren't really any specific symptoms that scream "acute kidney injury." But, you might see signs of whatever's causing the AKI, like vomiting and diarrhea if it's due to gastrointestinal losses. Urine production can be a clue – looking at how much urine is being made and how quickly it's decreasing. Other general symptoms can include feeling tired, nauseous, and even delirium. Patients might show signs of being hypovolemic (low fluid volume) or, on the flip side, fluid overloaded.
Acute Kidney Injury Diagnosis [6:02]
AKI is defined by an increase in serum creatinine by 26 micromoles per liter in 48 hours, an increase in creatinine by 1.5 times the baseline in seven days, or urine production of less than 0.5 milliliters per kilogram per hour for more than six hours. AKI is pretty common, affecting around 5% of hospital patients. It's usually spotted through blood tests showing high serum creatinine. These tests should also check electrolytes, since kidney problems can mess with electrolyte balance. A high urea to creatinine ratio often points to a pre-renal cause. Urine studies, like urine dips, can find proteinuria or microscopic hematuria. Urinalysis with microscopy can look for casts: brown or black casts may indicate acute tubular necrosis, red blood cell casts may indicate glomerulonephritis, and white blood cell casts may indicate acute interstitial nephritis. Electrolyte, creatinine, and urea concentrations in urine can also help figure out the cause, but diuretics can throw these off. Imaging, like ultrasound or CT scans, can help spot structural problems. In some cases, especially for intrinsic causes, a kidney biopsy might be needed to nail down the diagnosis.
Acute Kidney Injury Treatment [8:10]
Treatment for AKI depends on how severe it is and what's causing it. Usually, IV fluids are given to help kidney perfusion, unless the patient is already fluid overloaded. Any medications that could be causing the problem should be reviewed. The mnemonic "DAM" (Diuretics, ACE inhibitors/ARBs, Metformin, and NSAIDs) can help remember some of these. Metformin is included because it's excreted by the kidneys and can cause acidosis. But sometimes, even nephrotoxic meds might need to be continued, like diuretics for fluid overload from heart failure. Electrolyte imbalances should be corrected – for example, using calcium gluconate for hyperkalemia to stabilize the heart, along with insulin and dextrose to lower potassium while keeping blood glucose stable. If there's an obstruction, it should be relieved with a catheter. Urine output and fluid intake should be tracked, along with daily weights. Renal replacement therapy, like hemodialysis, might be needed for severe acidosis, hyperkalemia, drug intoxications, or when medical treatment isn't working.