TLDR;
This video provides a comprehensive guide on how to respond to choking and breathing emergencies, covering techniques for adults, children, and infants. It also explains the use of essential tools like bag valve masks and oxygen cylinders. Key points include:
- Recognising and responding to choking hazards in adults, children and infants.
- Performing CPR correctly, with adjustments for different age groups and special conditions like pregnancy.
- Using oxygen masks and bag valve masks effectively to support breathing.
Choking Emergency: Recognition and Response [0:09]
Choking is a life-threatening emergency requiring quick action. Partial obstruction is indicated by coughing or difficulty speaking, while complete obstruction prevents speech or coughing, often with bluish skin (cyanosis). For adults and children over one year, encourage coughing for partial obstructions. For complete obstructions, administer five back blows followed by five abdominal thrusts (Heimlich manoeuvre). For infants under one year, support them face down on your forearm and deliver five back blows, then turn them over and give five chest thrusts using two fingers. If the person becomes unresponsive, start CPR, checking the airway after every 30 chest compressions, and seek medical evaluation after clearing the obstruction due to potential complications.
Scenario: Six-Year-Old Choking on Candy [2:04]
A six-year-old child choking on candy is unable to speak or cough, indicating a complete obstruction. After five back blows fail to dislodge the candy, five abdominal thrusts are performed successfully. The child is then comforted and checked by a medical professional to rule out complications.
Scenario and Treatment of Mild Airway Obstruction [2:34]
A 40-year-old man is coughing after swallowing steak but can still speak in short phrases, indicating a mild airway obstruction. The man is coughing forcefully and wheezing, but is not showing signs of complete obstruction. Encourage forceful coughing and reassure him, avoiding physical intervention unless his condition worsens. Monitor for signs of worsening obstruction, such as difficulty breathing or cyanosis. If the obstruction persists or distress occurs after clearing it, advise consulting a medical professional. Avoid back blows or abdominal thrusts for mild obstructions, and never use a blind finger sweep.
Scenario and Treatment for Severe Airway Obstruction [4:57]
A seven-year-old child swallows a marble, causing a complete airway blockage, and is unable to cough, speak, or breathe, showing the universal choking sign and cyanosis. Confirm the severe obstruction by looking for key signs such as inability to speak, cough, or breathe. For children over one year, deliver five back blows followed by five abdominal thrusts, alternating until the object is expelled or the child becomes unresponsive. For infants under one year, support them face down and deliver five back blows, then turn them face up and deliver five chest thrusts, alternating until the object is expelled or the infant becomes unresponsive. If the patient becomes unresponsive, begin CPR immediately, checking the airway after 30 chest compressions. Seek medical attention even after the object is expelled to rule out complications.
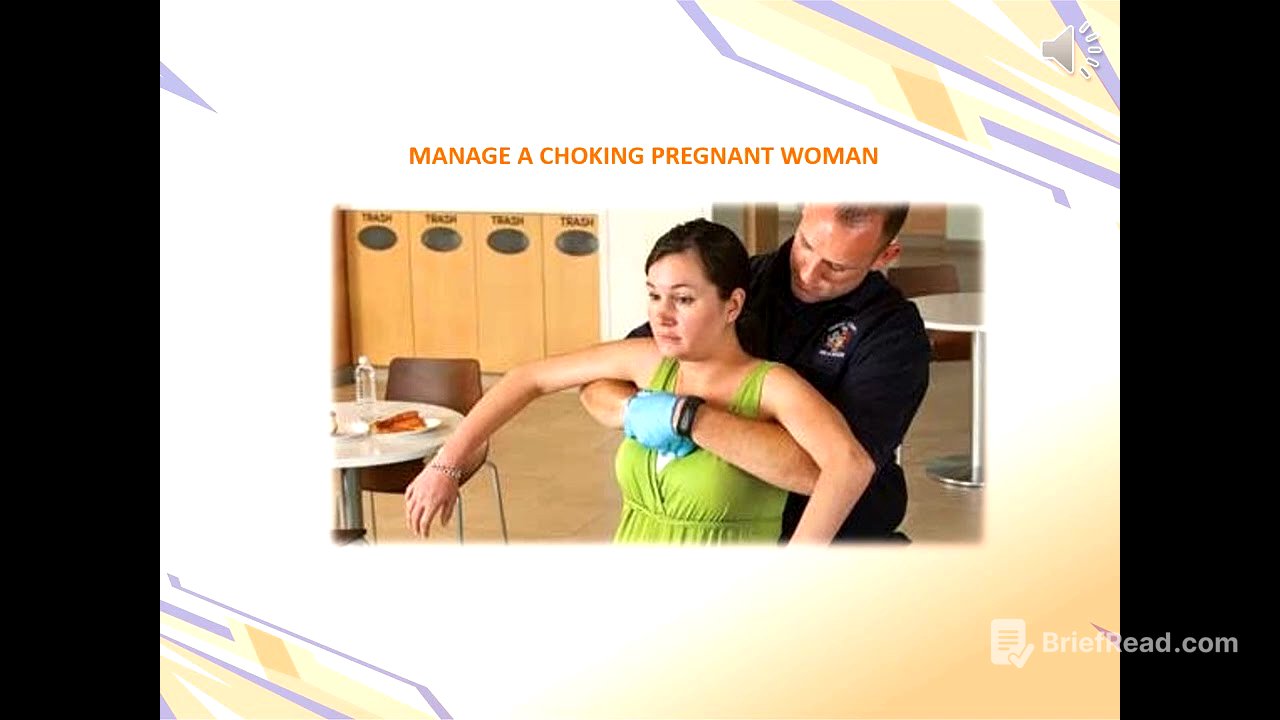
Scenario and Treatment: Managing a Choking Pregnant Woman [8:12]
A pregnant woman, approximately seven months along, is choking on bread and unable to speak, cough, or breathe, signalling a complete airway obstruction with cyanosis. Confirm the severe obstruction by recognising key signs such as inability to speak, cough, or breathe. Avoid abdominal thrusts due to the risk of harming the baby; instead, perform chest thrusts. Stand behind the woman, place arms under her armpits, form a fist, and deliver quick inward chest thrusts until the object is expelled or she becomes unresponsive. If unresponsive, lower her gently to the ground and begin CPR, focusing on chest compressions. Call for emergency services and ensure immediate medical attention for both the woman and the baby to rule out complications.
Choking in Infants: Step-by-Step Guide [11:13]
Choking in infants is a life-threatening emergency requiring swift action. Recognise the signs: silence, inability to cry, cough, or breathe, with cyanosis. Position the infant face down along your forearm, head lower than chest. Deliver five firm back blows between the shoulder blades. If unsuccessful, turn the infant face up and deliver five chest thrusts on the centre of their chest, just below the nipple line. Alternate back blows and chest thrusts until the object is expelled or the infant becomes unresponsive. If unresponsive, begin CPR with 30 chest compressions, check for the object in the airway, and attempt rescue breaths. Call emergency services even if the object is dislodged, to ensure medical evaluation for potential complications.
Clearing the Airway of an Unconscious Patient [16:52]
When encountering an unconscious patient struggling to breathe, the first step is to ensure a clear airway. Use the head-tilt-chin-lift technique to shift the tongue away and open the airway, checking for and removing visible obstructions. In cases of suspected spinal injury, use the jaw-thrust manoeuvre instead to avoid unnecessary spinal movement. If a foreign object is noticed, turn the patient onto their side and gently use a finger sweep to remove the obstruction, ensuring nothing falls deeper into the airway.
Bag Valve Mask (BVM): Overview and Usage [19:59]
A bag valve mask (BVM) is a vital resuscitation tool for providing positive pressure ventilation to patients with inadequate breathing. Key components include the face mask, pop-off valve, PEEP valve, self-inflating bag, oxygen inlet, reservoir bag, and one-way valve. Ensure a tight seal with the face mask to prevent air leakage. The pop-off valve prevents overinflation, while the PEEP valve maintains pressure in the lungs. Connect the BVM to an oxygen supply, typically at 15-18 litres per minute, and inflate the reservoir bag for high oxygen concentrations. Avoid hyperventilation by squeezing the bag slowly.
BVM Techniques: Single vs. Two Rescuers [24:04]
For single rescuers, use the C-grip technique to secure the mask while lifting the jaw. For two rescuers, use both hands to seal the mask, with thumbs pressing down and fingers lifting the jaw. To use a BVM, position the patient with a head-tilt-chin-lift (or jaw thrust if spinal injury is suspected), place the mask over the nose and mouth, attach oxygen, and ventilate while observing chest rise. Ensure a proper seal, avoid hyperventilation, and be aware that facial injuries or hair can hinder the seal.
Demonstration of Bag Valve Mask Technique [28:00]
The video demonstrates using a bag valve mask (BVM) with oxygen to deliver approximately 95% pure oxygen. The "anatis grip" involves placing two fingers on the mask, linking three fingers onto the jawbone, rolling the head back to open the airway, and pressing down for a good seal. The bag is squeezed gently for about one second per breath, looking for chest rise and fall, and feeling for any strain, gurgling, or bubbling, which indicate airway problems.
Understanding Oxygen Masks and Their Uses [29:41]
Oxygen masks are essential tools in first aid, each designed for specific needs. A nasal cannula is used for mild respiratory distress, delivering 24-44% oxygen at 1-6 litres per minute. A simple face mask is suitable for moderate distress, delivering 40-60% oxygen at 5-10 litres per minute. A non-rebreather mask is for severe distress, delivering 90-100% oxygen at 10-15 litres per minute. Ensure the reservoir bag is filled before use and monitor the patient's oxygen saturation.
Understanding Oxygen Cylinders and Regulators [33:04]
Oxygen cylinders store medical-grade oxygen under pressure. To use, inspect the cylinder, open the valve slowly, attach a regulator, connect tubing to a delivery device, and monitor pressure levels. Regulators reduce the cylinder's high pressure to a safe level and allow precise control of oxygen flow. To use, attach the regulator, open the valve slowly, set the flow rate (e.g., 2-15 litres per minute), and connect the delivery device.
Applying a Regulator to an Oxygen Tank: A Practical Guide [35:34]
The video demonstrates how to correctly apply a regulator to an oxygen tank. The regulator has two notches ("teeth") that must be inserted into the corresponding holes ("gums") on the tank. The regulator includes a gauge for pressure and a flow meter. After attaching the regulator, the tank is "cracked" open to check for leaks. Once properly attached and pressurised, oxygen tubing can be connected, and the flow rate adjusted. After use, the flow is closed, the tank locked, and the regulator depressurised before removal.
Oxygen Treatment: Indications, Safety, and Application [38:34]
Oxygen treatment is vital for patients with low oxygen levels due to respiratory distress, blood loss, high altitude, or toxic fumes exposure. High-concentration oxygen is safe for immediate use in emergencies for up to three hours, but prolonged use can lead to oxygen toxicity. A bag valve mask (BVM) allows rescuers to provide high oxygen concentrations, reducing the risk of cross-contamination. In practice, a first aider can use a portable oxygen tank and BVM to stabilise a mountain climber suffering from altitude sickness until evacuation.
Ensuring Effective Oxygen Delivery: Steps and Cautions [41:49]
To ensure effective oxygen delivery, start by ensuring a proper seal over the patient's nose and mouth. Set the oxygen cylinder's flow rate to 15 litres per minute to maximise oxygen delivery. Slowly open the main valve of the oxygen cylinder and check for leaks. Attach the regulator properly and select an appropriate mask based on the patient's condition. Explain the procedure to the patient to reduce anxiety. When using a bag valve mask (BVM), avoid overinflating the patient's lungs.
Questionnaires Reminder [45:17]
A reminder to complete the questionnaires in your notebook as part of the blended learning program. This activity is designed to deepen your understanding of the material covered so far and ensure that you can apply these critical first aid concepts in real life situations.
True and False Test Answers: Breathing Difficulties [47:07]
The video reviews answers to a true/false test on managing breathing difficulties. Key points: Partial airway obstruction doesn't always require immediate CPR; encourage coughing first. The universal choking sign is hands to the throat. Abdominal thrusts should be avoided on pregnant individuals and infants. The head-tilt-chin-lift is not for patients with spinal injuries; use the jaw thrust. A BVM can deliver nearly 100% oxygen with a reservoir and oxygen supply. Chest compressions during CPR should be about 120 per minute.
CPR: Definition, Importance, and Good Practices [52:10]
CPR (cardiopulmonary resuscitation) is an emergency procedure combining chest compressions and rescue breaths to restore blood circulation and breathing. Without oxygen, the brain suffers damage within 4-6 minutes, leading to cardiac arrest and potential death. CPR is critical in those first few moments. Performing CPR might cause minor harm like broken ribs, but the alternative is far worse. Combine chest compressions with rescue breaths whenever possible, especially for children. If you're getting tired, switch with another trained rescuer.
CPR: Positioning the Patient and Yourself [54:27]
Proper positioning is crucial for effective CPR. Move the patient onto a firm, flat surface and lay them flat on their back with arms at their sides. Ensure their head is positioned to maintain an open airway, using the head-tilt-chin-lift technique (unless spinal injury is suspected, in which case use the jaw thrust). Kneel beside the patient so that your shoulders are directly over their chest, keeping your elbows locked and using your upper body weight to press down. Call for help before starting CPR.
CPR: Hand Positioning for Chest Compressions [56:13]
Proper hand positioning is critical for effective chest compressions. Locate the compression point by tracing an imaginary line between the nipples; the centre of this line is where your hands should be placed on the sternum. Place the heel of one hand on the sternum, place your other hand on top of the first, and interlock your fingers. Your shoulders should be directly above your hands, and your elbows must remain locked. Compress the chest 5-6 cm (2-2.5 inches) for adults.
CPR Techniques: Adults, Children, and Infants [57:58]
CPR techniques vary for adults, children, and infants. For adults, use both hands to compress the chest 5-6 cm at a rate of 30 compressions followed by two rescue breaths. For children (ages 1-8), use one hand (or both if the child is larger) to compress about 1/3 of the chest depth, with a 15:2 compression-to-breath ratio when two rescuers are present. For infants (under one year), use two fingers to compress about 1/3 of the chest's diameter, also at a 15:2 ratio with two rescuers.
CPR: Single Rescuer Scenario [59:58]
As a single rescuer, place the heel of your hand on the sternum at the centre of the chest, interlock your fingers, and begin compressions, pushing hard and fast at 100-120 per minute. For every 30 compressions, give two rescue breaths, pinching the nose and sealing your mouth over theirs. Allow the chest to fully recoil after each compression. Continue CPR until help arrives, the patient shows signs of life, or you're too exhausted to continue.
CPR: Persistence Despite No Visible Recovery [1:01:06]
Even with no visible signs of recovery during CPR, continue unless the patient regains signs of life, professional help arrives, or you become physically unable to continue. Every attempt matters, and your efforts could be the difference between life and death.
Adult CPR for the Single Rescuer (Healthcare Professionals) [1:01:51]
The video demonstrates adult CPR for a single healthcare provider. After ensuring the scene is safe and donning gloves, the rescuer checks for responsiveness by tapping and shouting. If there's no response, EMS is activated. The rescuer then checks for normal breathing and a carotid pulse for no more than 10 seconds. If there's no normal breathing and no pulse, CPR is initiated with 30 chest compressions followed by two rescue breaths using a rescue mask.
CPR Scenario: Real-Time Demonstration with Two Rescuers [1:06:02]
A real-time scenario demonstrates two rescuers responding to a person not breathing. One rescuer assesses the situation and calls for help, while the other calls emergency services and retrieves an AED. Chest compressions are started, followed by rescue breaths. The AED is used, and its prompts are followed to deliver a shock. CPR continues with chest compressions and breaths.
Adult Basic Life Support Algorithm for Healthcare Providers [1:09:24]
The adult basic life support algorithm for healthcare providers starts with ensuring scene safety. Check for responsiveness, shout for help, and activate the emergency response system. Check for normal breathing and a pulse for no more than 10 seconds. If breathing and a pulse are present, monitor the patient. If there's no normal breathing but a pulse, provide rescue breathing. If there's no breathing or pulse, begin CPR with 30 chest compressions and two rescue breaths. Use an AED as soon as it's available, following its prompts.
Two-Rescuer CPR: Maximising Efficiency [1:11:51]
In a two-rescuer scenario, one kneels at the patient's head while the other positions themselves at the chest. The chest rescuer begins compressions at two compressions per second. After 30 compressions, the head rescuer delivers two breaths. Switch roles every five cycles to prevent fatigue.
Two-Rescuer Adult CPR for Healthcare Professionals [1:12:43]
The video demonstrates two-rescuer adult CPR for healthcare professionals. After assessing the scene and checking for responsiveness, one rescuer begins chest compressions while the other prepares to deliver rescue breaths using a bag valve mask. After 30 compressions, the rescuers switch roles to avoid fatigue, maintaining continuous CPR until an AED arrives or the patient revives.
CPR on a Child: Technique Adjustments [1:16:43]
When performing CPR on a child, adjust the technique to their smaller size. Use one hand for compressions (or both for larger children), compressing the chest to about 1/3 to 1/2 of its depth. Maintain the same rate as for adults (100-120 compressions per minute). If working alone, use the standard 30:2 ratio; with a second rescuer, switch to 15:2.
One-Rescuer Child CPR for Healthcare Providers [1:17:31]
The video demonstrates one-rescuer child CPR for healthcare providers. After ensuring scene safety and checking for responsiveness, the rescuer activates EMS. They then assess the child for normal breathing and a carotid pulse. If there's no breathing and no pulse, CPR is initiated with 30 compressions followed by two rescue breaths using a rescue mask.
CPR on an Infant: Precision and Technique [1:19:25]
Performing CPR on an infant requires precision. Check responsiveness by tapping the infant's feet and calling their name. Check circulation by feeling for a pulse on the brachial artery. For chest compressions, use your index and middle fingers on the centre of the chest below the nipple line, compressing to about 1/3 to 1/2 the chest depth at 100-120 compressions per minute. Use a 30:2 ratio if alone, or 15:2 with a second rescuer. Keep the head in a neutral position and cover both the nose and mouth for rescue breaths.
One-Rescuer Infant CPR for Healthcare Providers [1:22:19]
The video demonstrates one-rescuer infant CPR for healthcare providers. After ensuring scene safety and checking for responsiveness, the rescuer activates EMS. They then check for breathing and a brachial pulse. If there's no breathing and no pulse, CPR is initiated with two fingers placed on the lower third of the sternum, compressing to approximately one-third of the chest depth at 100-120 compressions per minute, followed by two rescue breaths using an appropriately sized CPR shield.
Paediatric Basic Life Support Algorithm for Healthcare Providers (Single Rescuer) [1:25:46]
The paediatric basic life support algorithm for healthcare providers (single rescuer) involves ensuring scene safety, checking for responsiveness, and activating the emergency response system. Check for breathing and pulse simultaneously for no more than 10 seconds. If there's normal breathing and a pulse, monitor the child. If there's no normal breathing but a pulse, provide rescue breathing. If there's no breathing or pulse, start CPR with 30 compressions and two breaths. Use an AED as soon as available, following its prompts.
Paediatric Basic Life Support Algorithm for Healthcare Providers (Two or More Rescuers) [1:28:27]
The paediatric basic life support algorithm for two or more rescuers involves ensuring scene safety, checking for responsiveness, and having one rescuer activate the emergency response system while the other stays with the child. Check for breathing and pulse simultaneously. If there's normal breathing and a pulse, monitor the child. If there's no normal breathing but a pulse, provide rescue breathing. If there's no breathing or pulse, start CPR, switching to a 15:2 compression-to-breath ratio once the second rescuer returns. Use an AED as soon as available, following its prompts.
CPR: Critical Notes for Effective Execution [1:30:51]
Start CPR immediately after confirming unresponsiveness and lack of breathing. CPR may cause minor injuries like broken ribs, but these are outweighed by the need to save the patient's life. Before rescue breaths, check for visible airway obstructions. If rescue breaths can't be provided, perform hands-only CPR. For children and infants, deliver both compressions and breaths. If no pulse is felt, assume cardiac arrest and start chest compressions right away.
CPR: Best Practices for Effective Resuscitation [1:32:41]
To perform CPR effectively, maintain proper compression depth (5-6 cm for adults, 1/3 to 1/2 chest depth for children and infants), ensure full chest recoil after each compression, and keep a steady compression rate of 100-120 per minute. Maintain correct hand placement, minimise interruptions between compressions and rescue breaths, switch rescuers every five cycles to avoid fatigue, and blow gently when giving rescue breaths to prevent overinflating the lungs.
Hands-Only CPR: A Vital Technique [1:34:36]
Hands-only CPR involves focusing solely on chest compressions, maintaining circulation until professional help arrives. It's effective in adult sudden cardiac arrest, especially if witnessed. It's less effective for children and infants, as their cardiac arrests are often respiratory-related. Hands-only CPR is encouraged if a rescuer is unable or unwilling to perform rescue breaths.
Questionnaires Reminder [1:35:57]
A reminder to complete the questionnaires in your notebook as part of the blended learning program. This activity is designed to deepen your understanding of the material covered so far and ensure that you can apply these critical first aid concepts in real life situations.
True or False CPR Questionnaire with Explanations [1:37:47]
The video reviews answers to a true/false CPR questionnaire. Key points: Chest compressions should be 100-120 per minute. Start CPR immediately after confirming unresponsiveness and lack of breathing. Adult CPR compressions should be 5-6 cm deep. Rescue breaths aren't always necessary during hands-only CPR. Don't stop CPR until help arrives or you're physically unable to continue. Use two fingers for infant CPR compressions. AEDs can be used by anyone, even without training. For children, compress the chest to about 1/3 to 1/2 its depth. Resume CPR immediately after delivering a shock with an AED. CPR is less effective for children and infants without rescue breaths.